YOUR SPECIALIST FOR SHORT-STEM TOTAL HIP ARTHROPLASTY PROF. DR. MED K.P. KUTZNER - GERMANY
YOUR SPECIALIST FOR SHORT-STEM TOTAL HIP ARTHROPLASTY PROF. DR. MED K.P. KUTZNER - GERMANY


Short-stem total hip arthroplasty is closely associated with minimally invasive surgical techniques. The use of smaller incisions aims to reduce soft tissue disruption, leading to decreased postoperative pain, accelerated recovery, and improved patient satisfaction. Minimally invasive techniques associated with short-stem THA contribute to shorter hospital stays, and faster overall recovery.
The adoption of short-stem THA techniques requires a learning curve for surgeons. Mastery of the technique and familiarity with implant-specific considerations are essential for success.

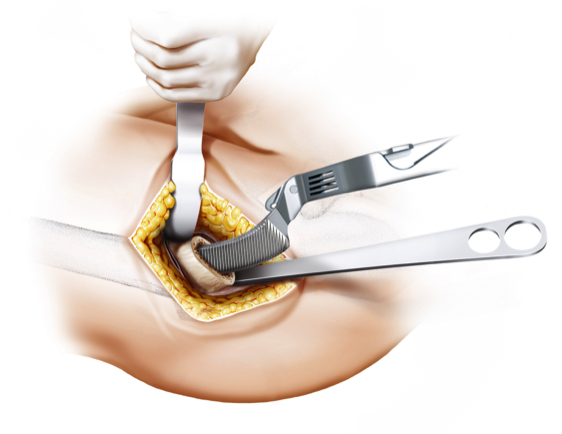
Minimally Invasive Approaches
Short-stem total hip arthroplasty (THA) is often associated with minimally invasive surgical (MIS) techniques, representing a departure from the more traditional, larger-incision approaches. Minimally invasive surgery aims to reduce soft tissue disruption, decrease postoperative pain, accelerate recovery, and enhance overall patient satisfaction.
The use of smaller incisions in MIS for short-stem THA requires specialized training and expertise on the part of the surgeon. This approach allows for a more tissue-sparing procedure, potentially leading to shorter hospital stays and quicker rehabilitation for the patient. However, the adoption of minimally invasive techniques should be balanced with ensuring proper exposure, component positioning, and achieving optimal outcomes.
Femoral Neck Preservation Techniques
Preservation of the femoral neck is a key consideration in short-stem THA, and various techniques aim to achieve this goal. The femoral neck is critical for maintaining the biomechanics of the hip joint and ensuring proper load transfer. Preserving the natural anatomy of the femoral neck is particularly relevant in short-stem designs, where stability and functionality depend on maintaining these anatomical features.
Calcar-guided short stems, for example, are designed to preserve the calcar region of the femoral neck, contributing to enhanced stability and load distribution. Techniques that prioritize femoral neck preservation not only aim to replicate the natural biomechanics of the hip joint but also play a role in improving long-term outcomes and reducing the risk of complications.
Customization and Personalization in Short-Stem Surgery
One of the notable advantages of short-stem THA is the ability to customize and personalize the surgical approach based on individual patient anatomy. Short-stem implants often come with modular options, allowing surgeons to choose components that closely match the patient's unique femoral morphology.
Customization extends beyond implant selection and involves tailoring the surgical technique to the patient's specific needs. Computer-assisted navigation and robotic surgery are emerging technologies that offer additional precision in implant placement, further enhancing the level of customization in short-stem THA.
Tips for Surgeon Proficiency
Proficiency in short-stem THA requires a learning curve for surgeons, as the techniques and considerations differ from those associated with traditional long-stem implants. To optimize outcomes and minimize potential complications, surgeons adopting short-stem THA should consider the following:
The proficiency of the surgeon in short-stem THA is instrumental in achieving optimal outcomes, and ongoing advancements in surgical techniques will continue to refine the approach.
Calcar-guided short-stem total hip arthroplasty (THA) represents one of the most important evolutions in modern cementless hip replacement. Unlike conventional straight stems, this philosophy allows individualized implantation that follows the patient’s anatomy rather than forcing the anatomy to adapt to the implant.
A key insight that emerged from clinical experience and scientific investigation was that:
The same short stem can function biomechanically in very different ways depending on how it is implanted.
To address this variability, Kutzner et al. introduced a structured classification system that differentiates anchorage strategies in calcar-guided short-stem THA. This system is now known as the:
👉 Kutzner Classification
Rather than describing implant design, it describes the type of fixation achieved.
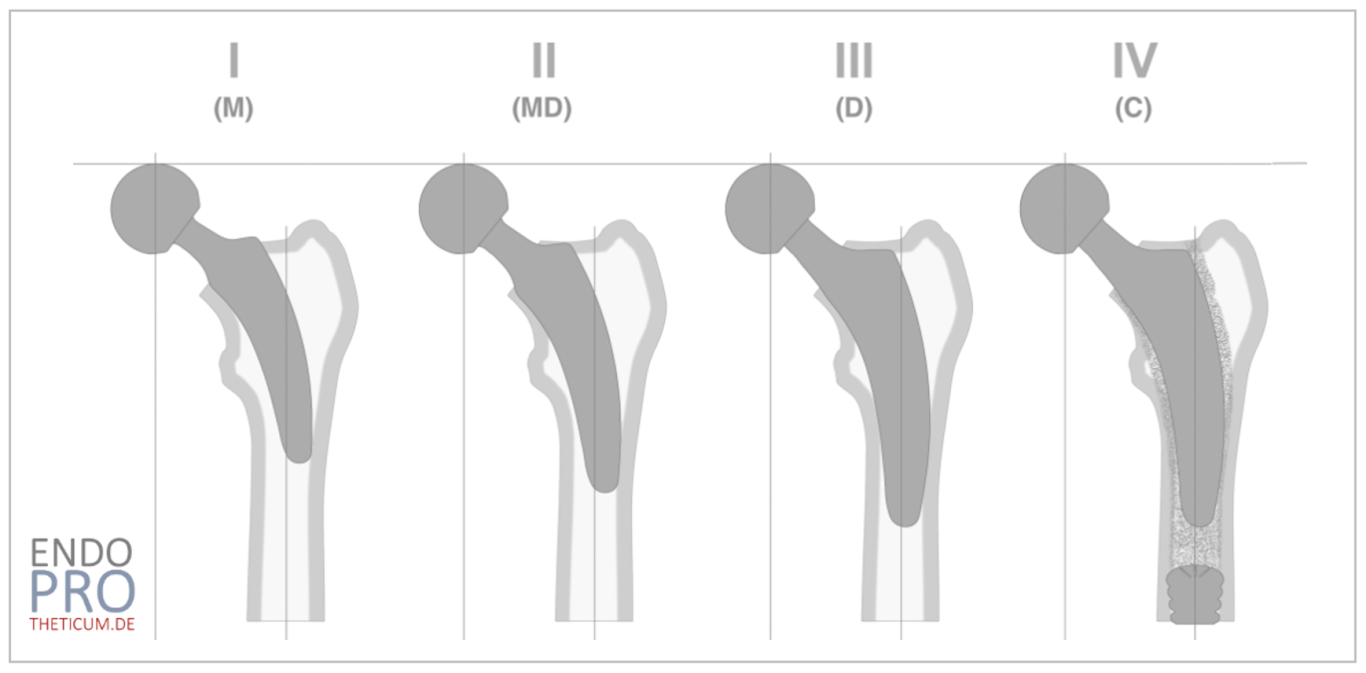
The Kutzner Classification distinguishes four different anchorage concepts in calcar-guided short-stem THA:
Group I – Metaphyseal fixation
Group II – Meta-diaphyseal fixation
Group III – Diaphyseal fixation
Group IV – Cemented fixation
Together, they describe a proximal-to-distal continuum of load transfer.
Group I – Metaphyseal Fixation
Group I represents the purest form of short-stem implantation.
Here, stability is achieved exclusively in the metaphysis. The implant is anchored proximally, primarily in the calcar region and surrounding cancellous bone.
There is little to no engagement of the diaphyseal canal.
Biomechanically, this allows:
Physiological proximal load transfer
Reduced stress shielding
Maximum preservation of bone
Group I fixation is typically achievable in patients with:
Good bone quality
Normal proximal femoral anatomy
Sufficient metaphyseal support
Whenever possible, this fixation type is considered the preferred strategy because it maintains the core advantages of short-stem arthroplasty.
Group II – Meta-Diaphyseal Fixation
In Group II, fixation extends beyond the metaphysis into the transitional zone between metaphysis and diaphysis.
The implant still relies on proximal support, but gains additional stability from partial distal contact.
This creates a hybrid fixation pattern.
Load transfer remains partly physiological, but with increased structural support.
Group II fixation is often encountered in:
Moderate bone quality
Slight anatomical variations
Situations requiring enhanced rotational stability
This anchorage type represents a balanced compromise between proximal preservation and mechanical safety.
Group III – Diaphyseal Fixation
In Group III, primary stability shifts to the diaphysis.
Although the implant remains a short stem by design, functionally it behaves more like a conventional stem with distal support.
Metaphyseal fixation becomes secondary.
This strategy may be necessary in:
Poor metaphyseal bone quality
Structural deformities
Challenging primary cases
Load transfer is now predominantly directed toward the femoral shaft.
While this reduces the degree of physiological proximal loading, it ensures mechanical stability in demanding situations.
Group IV – Cemented Fixation
Group IV describes cemented short-stem fixation.
This option is used when neither metaphyseal nor diaphyseal anchorage can ensure reliable stability.
Cement fixation allows the surgeon to maintain the bone-preserving geometry of short stems while compensating for compromised bone quality.
Typical indications include:
Osteoporotic bone
Advanced age
Complex femoral morphology
Load transfer occurs via the cement mantle rather than direct bone contact.
This expands the indication spectrum of calcar-guided short stems beyond ideal bone conditions.
The Importance of Surgical Technique
A central insight of the Kutzner Classification is that fixation type is determined primarily by technique rather than implant design.
By modifying:
Osteotomy level
Implant alignment
The surgeon can intentionally influence anchorage behavior.
For example:
High osteotomy → promotes metaphyseal fixation
Lower osteotomy → increases distal engagement
Thus, the classification serves not only as a descriptive system but also as:
A planning tool
A documentation framework
A teaching concept
Read more here: The Kutzner Classification in calcar-guided short-stem THA

Successful implementation of short-stem THA requires surgeon expertise and familiarity with the specific challenges and advantages associated with these implants. Adequate training and continuous education are essential for optimizing outcomes.
Wir benötigen Ihre Zustimmung zum Laden der Übersetzungen
Wir nutzen einen Drittanbieter-Service, um den Inhalt der Website zu übersetzen, der möglicherweise Daten über Ihre Aktivitäten sammelt. Bitte überprüfen Sie die Details in der Datenschutzerklärung und akzeptieren Sie den Dienst, um die Übersetzungen zu sehen.